50 GPT-5.5 Prompts for Healthcare Professionals: Clinical Decision Support, Medical Documentation, Patient Communication, and Research Analysis

50 GPT-5.5 Prompts for Healthcare Professionals: Clinical Decision Support, Medical Documentation, Patient Communication, and Research Analysis
By Markos Symeonides | June 20, 2026
Healthcare professionals are under more pressure than ever. Between expanding patient loads, increasingly complex documentation requirements, evolving clinical guidelines, and the demand for personalized patient communication, the cognitive burden on physicians, nurses, researchers, and administrators has reached a critical point. GPT-5.5 — OpenAI’s most capable and clinically nuanced model to date — is changing that equation in measurable, practical ways.
This guide is not a theoretical overview of AI in medicine. It is a working toolkit: 50 production-ready prompts organized by clinical function, each designed to be copied, adapted, and deployed immediately. Every prompt includes context variables in [BRACKETS] so you can customize them to your specialty, patient population, or institution’s documentation standards. Whether you’re a hospitalist drafting discharge summaries at midnight, a clinical researcher synthesizing RCT data, or a patient educator building health literacy materials, these prompts will save you time without sacrificing clinical accuracy.
Before diving in, one critical caveat: GPT-5.5 is a powerful reasoning and language tool, not a licensed medical practitioner. Every output must be reviewed by a qualified clinician before being used in patient care decisions. These prompts are designed to accelerate and support clinical workflows, not replace clinical judgment. With that established, let’s get to work.
Section 1: Clinical Decision Support Prompts
Clinical decision support is where GPT-5.5 demonstrates its most impressive capabilities. The model’s ability to synthesize differential diagnoses, identify drug interactions, flag contraindications, and reason through complex clinical presentations makes it a powerful second-opinion tool — particularly in resource-limited settings or during off-hours when specialist consultation isn’t immediately available. These prompts are structured to elicit structured, evidence-referenced reasoning rather than vague generalities.
Prompt 1: Differential Diagnosis Generation
You are a senior internal medicine consultant. A [AGE]-year-old [BIOLOGICAL_SEX] patient presents with the following chief complaint and history:
Chief Complaint: [CHIEF_COMPLAINT]
History of Present Illness: [HPI_NARRATIVE]
Relevant Past Medical History: [PMH]
Current Medications: [MEDICATION_LIST]
Relevant Labs/Imaging: [LAB_AND_IMAGING_RESULTS]
Vital Signs: [VITALS]
Generate a ranked differential diagnosis with at least 8 conditions. For each condition:
1. Explain why this presentation is consistent with the diagnosis
2. Identify the single most important distinguishing test or finding
3. Assign a likelihood tier: High / Moderate / Low / Must-Not-Miss
4. Note any red flag features that require urgent action
Format as a structured table followed by a brief narrative synthesis. Cite relevant clinical guidelines where applicable (e.g., AHA, IDSA, UpToDate-level evidence).Prompt 2: Drug Interaction Checker with Clinical Context
You are a clinical pharmacist with expertise in polypharmacy management. A patient is currently taking the following medications:
[MEDICATION_LIST_WITH_DOSES_AND_FREQUENCIES]
The treating physician wants to add: [NEW_MEDICATION] at [PROPOSED_DOSE].
Patient context:
- Age: [AGE]
- Weight: [WEIGHT_KG]
- Renal function: eGFR [EGFR_VALUE]
- Hepatic function: [NORMAL/MILD/MODERATE/SEVERE_IMPAIRMENT]
- Relevant comorbidities: [COMORBIDITIES]
Perform a comprehensive drug interaction analysis:
1. Identify all clinically significant interactions (CYP450, QTc prolongation, serotonin syndrome risk, bleeding risk, etc.)
2. Rate each interaction: Contraindicated / Major / Moderate / Minor
3. Provide the pharmacological mechanism for each major or contraindicated interaction
4. Suggest evidence-based alternatives if a contraindicated combination exists
5. Recommend monitoring parameters if the combination proceeds
Base your analysis on FDA labeling, Lexicomp-equivalent evidence, and current clinical practice guidelines.Prompt 3: Sepsis Risk Stratification
You are an emergency medicine physician. Evaluate the following patient for sepsis risk using qSOFA, SOFA, and NEWS2 criteria:
Patient Data:
- Temperature: [TEMP_C]
- Heart Rate: [HR_BPM]
- Respiratory Rate: [RR_PER_MIN]
- Blood Pressure: [BP_SYSTOLIC]/[BP_DIASTOLIC]
- SpO2: [SPO2_PERCENT] on [O2_DELIVERY]
- GCS or mental status: [GCS_OR_DESCRIPTION]
- Lactate: [LACTATE_MMOL_L]
- WBC: [WBC_K_UL]
- Creatinine: [CREATININE_MG_DL] (baseline: [BASELINE_CREATININE])
- Bilirubin: [BILIRUBIN_MG_DL]
- Platelets: [PLATELETS_K_UL]
- Known/suspected source of infection: [INFECTION_SOURCE]
1. Calculate qSOFA, SOFA, and NEWS2 scores with component breakdown
2. Assign Sepsis-3 classification: SIRS / Sepsis / Septic Shock
3. Recommend immediate management steps per Surviving Sepsis Campaign 1-hour bundle
4. Identify any atypical features that might suggest an alternative diagnosis
5. Flag any medication contraindications based on the clinical picturePrompt 4: Antibiotic Stewardship Recommendation
You are an infectious disease specialist and antibiotic stewardship consultant. Review the following case and provide antibiotic guidance:
Diagnosis: [CONFIRMED_OR_SUSPECTED_DIAGNOSIS]
Culture results: [CULTURE_SOURCE_AND_ORGANISM_WITH_SENSITIVITIES]
Patient weight: [WEIGHT_KG]
Renal function: eGFR [EGFR_VALUE]
Hepatic function: [STATUS]
Allergies: [ALLERGY_LIST_WITH_REACTION_TYPE]
Current empiric antibiotic: [CURRENT_ANTIBIOTIC_DOSE_ROUTE]
Duration of current therapy: [DAYS_ON_CURRENT_THERAPY]
Clinical response: [IMPROVING/STABLE/DETERIORATING]
Provide:
1. De-escalation or escalation recommendation with rationale
2. Optimal agent, dose, route, and duration based on IDSA guidelines and local resistance patterns
3. Therapeutic drug monitoring recommendations if applicable (e.g., vancomycin AUC/MIC)
4. Oral step-down criteria if IV therapy is current
5. Duration of therapy recommendation with evidence basisPrompt 5: Preoperative Risk Assessment
You are an anesthesiologist performing a preoperative evaluation. Assess surgical risk for the following patient:
Planned procedure: [PROCEDURE_NAME] — [ELECTIVE/URGENT/EMERGENT]
Surgical risk category: [LOW/INTERMEDIATE/HIGH_RISK_SURGERY]
Patient profile:
- Age: [AGE], [BIOLOGICAL_SEX]
- BMI: [BMI]
- Functional capacity: [METS — describe activity tolerance]
- Cardiac history: [CARDIAC_CONDITIONS]
- Pulmonary history: [PULMONARY_CONDITIONS]
- Metabolic/endocrine: [DIABETES_THYROID_ETC]
- Current medications: [MEDICATIONS]
- Prior anesthetic complications: [YES/NO — describe if yes]
- Recent ECG: [FINDINGS_OR_NORMAL]
- Recent echo: [FINDINGS_OR_NOT_AVAILABLE]
- Labs: [RELEVANT_LABS]
Using ACC/AHA 2014 perioperative guidelines and RCRI scoring:
1. Calculate RCRI score with component breakdown
2. Estimate 30-day MACE risk
3. Recommend whether additional cardiac testing is indicated before surgery
4. Identify medications requiring perioperative management (beta-blockers, anticoagulants, antiplatelets, diabetes medications, steroids)
5. Provide ASA physical status classification with justificationPrompt 6: Pediatric Dosing Calculator Prompt
You are a pediatric clinical pharmacist. Calculate appropriate medication dosing for the following pediatric patient:
Patient: [AGE_YEARS_MONTHS], [WEIGHT_KG], [HEIGHT_CM]
BSA (if calculated): [BSA_M2]
Diagnosis requiring treatment: [DIAGNOSIS]
Medication to dose: [MEDICATION_NAME]
Indication: [SPECIFIC_INDICATION]
Renal function: [NORMAL/SPECIFY_EGFR_OR_SCRUM_CREATININE]
Hepatic function: [NORMAL/ABNORMAL]
Known allergies: [ALLERGIES]
Provide:
1. Weight-based dose calculation (mg/kg) with reference range
2. BSA-based dose if applicable (oncology, certain antibiotics)
3. Maximum dose ceiling and rationale
4. Appropriate formulation for age (liquid, crushable tablet, etc.)
5. Frequency and total daily dose
6. Monitoring parameters specific to this patient's age and weight
7. Any age-specific contraindications or precautions
8. Source: cite Harriet Lane, Lexicomp Pediatrics, or relevant FDA labeling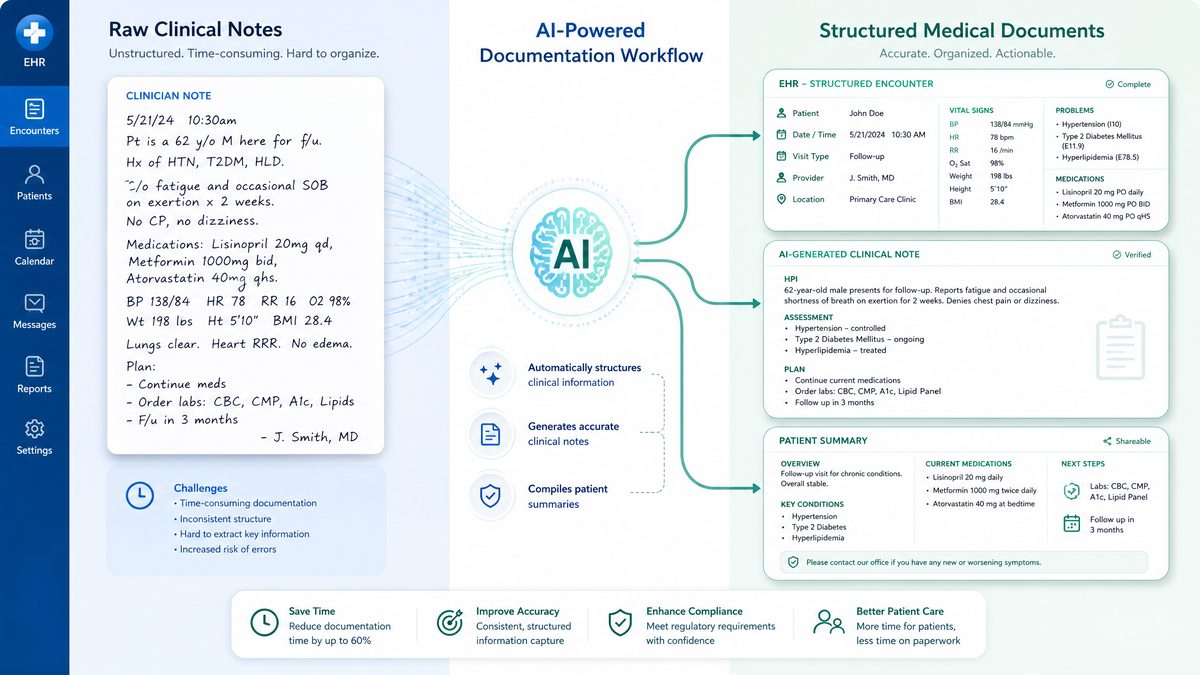
Section 2: EHR Documentation and Medical Writing Prompts
Documentation burden is one of the leading contributors to physician burnout. Studies published in the Annals of Internal Medicine consistently show that for every hour of direct patient care, physicians spend nearly two hours on EHR documentation. GPT-5.5’s structured output capabilities make it exceptionally well-suited for generating SOAP notes, discharge summaries, referral letters, and prior authorization narratives — all formatted to institutional standards. These prompts are designed to produce documentation that is clinically precise, legally defensible, and ready for attending physician review and signature.
It’s worth noting that many health systems are now integrating GPT-5.5 directly into their EHR platforms via API, allowing ambient documentation workflows where the model listens to patient encounters and generates structured notes in real time. Even without native integration,
Healthcare organizations handling protected health information must maintain rigorous security standards. Our Codex Security Prompts Masterclass provides 30 production-ready prompts for automated threat modeling and vulnerability remediation that complement clinical AI deployments by ensuring HIPAA-compliant code practices across medical software systems. Codex Security Prompts Masterclass: 30 Production-Ready Prompts.
these prompts can be used with copy-paste efficiency to dramatically reduce after-hours charting time.
Prompt 7: SOAP Note Generation
You are a [SPECIALTY] physician. Generate a complete, billable SOAP note based on the following encounter information:
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Visit type: [NEW_PATIENT/ESTABLISHED_PATIENT] — [IN_PERSON/TELEHEALTH]
Chief complaint: [CHIEF_COMPLAINT]
Encounter narrative: [PASTE_DICTATED_OR_TYPED_ENCOUNTER_NOTES_HERE]
Vital signs: [VITALS]
Relevant labs reviewed: [LABS]
Imaging reviewed: [IMAGING]
Current medications: [MEDICATION_LIST]
Generate a SOAP note that:
1. Follows standard SOAP format (Subjective, Objective, Assessment, Plan)
2. Includes a complete ROS (Review of Systems) based on the chief complaint — mark systems as positive or negative
3. Documents physical exam findings consistent with the encounter
4. Provides Assessment with primary diagnosis (ICD-10 code) and up to 3 secondary diagnoses
5. Creates a numbered Problem List with specific management steps for each
6. Includes MDM (Medical Decision Making) complexity level: Straightforward / Low / Moderate / High
7. Formats for [EPIC/CERNER/ATHENA/OTHER_EHR] documentation standards
8. Flags any missing elements that require physician completion before signingPrompt 8: Hospital Discharge Summary
You are a hospitalist physician. Write a comprehensive hospital discharge summary using the following information:
Patient demographics: [AGE], [BIOLOGICAL_SEX], [MRN_OPTIONAL]
Admission date: [DATE] | Discharge date: [DATE]
Admitting diagnosis: [DIAGNOSIS]
Discharge diagnosis (primary): [FINAL_DIAGNOSIS]
Secondary diagnoses addressed during admission: [LIST]
Hospital course narrative: [PASTE_PROGRESS_NOTE_SUMMARIES_OR_BRIEF_NARRATIVE]
Procedures performed: [PROCEDURE_LIST_WITH_DATES]
Consultations: [SPECIALTY_AND_KEY_RECOMMENDATIONS]
Significant labs/imaging: [KEY_RESULTS_WITH_DATES]
Discharge condition: [STABLE/FAIR/GUARDED]
Discharge disposition: [HOME/SNF/REHAB/HOSPICE]
Discharge medications: [COMPLETE_MEDICATION_LIST_WITH_DOSES]
Medications changed from admission: [NEW/STOPPED/DOSE_CHANGED]
Allergies: [ALLERGY_LIST]
Follow-up plan: [APPOINTMENTS_SCHEDULED]
Pending results at discharge: [LIST_WITH_RESPONSIBLE_PROVIDER]
Patient/family education provided: [TOPICS_COVERED]
Write a discharge summary that:
1. Follows JCAHO/Joint Commission standards for completeness
2. Clearly explains the reason for admission, hospital course, and discharge plan
3. Highlights medication changes with rationale in a separate section
4. Includes a "Critical Pending Results" section with follow-up responsibility assigned
5. Is written at a level appropriate for receiving providers (PCPs, SNF staff)
6. Flags any unresolved issues requiring outpatient workupPrompt 9: Prior Authorization Letter
You are a physician writing a prior authorization request letter to a commercial insurance payer. Generate a compelling, evidence-based prior authorization letter for:
Requested medication/procedure: [MEDICATION_OR_PROCEDURE]
Diagnosis (ICD-10): [DIAGNOSIS_WITH_CODE]
Patient profile: [AGE], [BIOLOGICAL_SEX], relevant comorbidities: [LIST]
Clinical justification:
- Duration of condition: [DURATION]
- Previous treatments tried and failed: [LIST_WITH_DURATION_AND_REASON_FOR_FAILURE]
- Current disease severity: [SEVERITY_METRICS_SCORES_LABS]
- Why requested treatment is medically necessary: [CLINICAL_RATIONALE]
- Relevant guidelines supporting use: [GUIDELINE_REFERENCES]
The letter must:
1. Open with a clear statement of medical necessity
2. Document step therapy compliance (prior treatment failures)
3. Reference FDA approval status and relevant clinical trial data (cite specific trials)
4. Address likely payer objections preemptively (e.g., formulary alternatives)
5. Include urgency statement if applicable
6. Close with specific appeal to payer's own coverage criteria language
7. Be formatted for fax submission with appropriate signature blockPrompt 10: Referral Letter to Specialist
You are a primary care physician writing a specialist referral letter. Generate a professional, complete referral letter:
Referring physician: [NAME, CREDENTIALS, PRACTICE_NAME, CONTACT]
Receiving specialist: [SPECIALTY] at [PRACTICE_OR_HOSPITAL]
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Reason for referral: [SPECIFIC_QUESTION_OR_CONCERN]
Clinical summary:
- Relevant history: [HPI_SUMMARY]
- Pertinent PMH/PSH: [HISTORY]
- Current medications: [LIST]
- Allergies: [LIST]
- Relevant exam findings: [FINDINGS]
- Relevant labs/imaging (with dates and values): [RESULTS]
- Treatments already attempted: [LIST_WITH_OUTCOMES]
Specific questions for specialist:
1. [QUESTION_1]
2. [QUESTION_2]
3. [QUESTION_3]
Urgency: [ROUTINE/URGENT/EMERGENT — within X days/weeks]
Write a letter that is concise (under 400 words), clinically complete, avoids redundancy, and gives the specialist everything they need to prepare for the consultation without requiring additional record requests.Prompt 11: Operative Report Narrative
You are a [SURGICAL_SPECIALTY] surgeon. Generate an operative report narrative based on the following procedural data:
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Procedure: [PROCEDURE_NAME]
Indication: [INDICATION]
Surgeon: [SURGEON_NAME] | Assistant: [ASSISTANT_NAME_OR_NONE]
Anesthesia: [GENERAL/REGIONAL/LOCAL] — administered by [ANESTHESIOLOGIST_NAME]
Date/time: [DATE], [START_TIME] to [END_TIME]
Estimated blood loss: [EBL_ML]
Fluids administered: [IV_FLUIDS_ML]
Specimens sent: [SPECIMEN_DESCRIPTION_AND_DESTINATION]
Drains placed: [YES/NO — describe]
Complications: [NONE/DESCRIBE]
Procedural steps performed: [NUMBERED_LIST_OF_STEPS_AS_DICTATED]
Findings: [INTRAOPERATIVE_FINDINGS]
Closure: [CLOSURE_TECHNIQUE]
Generate a formal operative report narrative that:
1. Follows standard surgical operative report format
2. Uses appropriate surgical terminology for [SURGICAL_SPECIALTY]
3. Documents consent, patient positioning, prep, and draping
4. Describes each procedural step in logical, defensible sequence
5. Clearly documents any intraoperative decision-making or deviations from planned procedure
6. Is formatted for direct EHR entrySection 3: Patient Communication and Health Education Prompts
Health literacy remains one of the most underaddressed challenges in American healthcare. The National Assessment of Adult Literacy reports that approximately 36% of U.S. adults have basic or below-basic health literacy skills, meaning standard patient education materials written at a 10th-grade level are effectively inaccessible to more than a third of patients. GPT-5.5 excels at translating complex medical information into plain language without sacrificing clinical accuracy — a capability that has direct, measurable impact on medication adherence, informed consent quality, and patient satisfaction scores.
These prompts are built around the principle of “teach-back readiness” — every output should be written so that a patient can explain the key concepts back to their provider. For institutions using patient portal messaging systems,
Effective medical documentation requires precise prompt engineering techniques. Our guide to advanced prompt patterns for writing demonstrates structural approaches and working examples that healthcare professionals can adapt for generating clear patient education materials, discharge summaries, and clinical correspondence. Advanced Prompt Patterns for writing: Working Examples.
these prompts can be adapted to generate portal-ready messages that pass automated plain-language readability checks.
Prompt 12: Patient Education Handout
You are a health educator creating a patient education handout. Write a comprehensive but accessible handout about:
Condition/Topic: [CONDITION_OR_TOPIC]
Target audience: [AGE_GROUP], primary language: [LANGUAGE], estimated health literacy: [LOW/MODERATE/HIGH]
Reading level target: [6TH_GRADE/8TH_GRADE] (Flesch-Kincaid)
Format: [PRINT_HANDOUT/PATIENT_PORTAL/DISCHARGE_INSTRUCTION]
The handout must cover:
1. What is [CONDITION] — explained in plain language with one simple analogy
2. What causes it (avoid jargon; use everyday comparisons)
3. Symptoms to watch for — presented as a "When to call your doctor" checklist
4. How it is treated — explain the purpose of each medication/intervention in one sentence
5. What the patient can do at home — 5 specific, actionable steps
6. When to go to the emergency room — clear red flag criteria
7. Questions to ask your doctor at your next visit — 3 pre-written questions
Formatting requirements:
- Use short paragraphs (3 sentences maximum)
- Use bullet points for lists
- Bold all critical action items
- Avoid all medical abbreviations unless defined immediately after first use
- Include a "Key Words to Know" glossary of up to 5 terms at the bottomPrompt 13: Informed Consent Explanation
You are a physician preparing a patient for informed consent discussion for:
Procedure: [PROCEDURE_NAME]
Patient: [AGE]-year-old [BIOLOGICAL_SEX] with [RELEVANT_COMORBIDITIES]
Patient's primary language: [LANGUAGE]
Health literacy level: [LOW/MODERATE/HIGH]
Specific patient concerns noted: [PATIENT_CONCERNS_IF_KNOWN]
Generate a plain-language informed consent explanation that covers:
1. What the procedure involves — described in 3-5 sentences without medical jargon
2. Why this procedure is being recommended for this specific patient
3. The most common risks (>1% incidence) — listed plainly
4. The rare but serious risks — listed with approximate frequency
5. What happens if the patient chooses NOT to have the procedure
6. Available alternatives with brief pros/cons comparison
7. What recovery looks like — realistic timeline and activity restrictions
8. Three questions the patient should feel empowered to ask before signing
This explanation will be used verbally by the physician AND as a written supplement to the formal consent form. It is not a replacement for the legal consent document.Prompt 14: Medication Instruction Sheet
You are a clinical pharmacist creating a patient-facing medication instruction sheet for:
Medication: [MEDICATION_NAME] [DOSE] [FORMULATION]
Indication: [WHY_PRESCRIBED — in plain language]
Prescribing physician: [PHYSICIAN_NAME]
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Other current medications: [RELEVANT_MEDICATIONS_FOR_INTERACTION_COUNSELING]
Special populations: [PREGNANCY/BREASTFEEDING/RENAL_IMPAIRMENT/NONE]
Create a medication instruction sheet that includes:
1. What this medication is and why you are taking it (2-3 plain sentences)
2. Exactly how to take it: dose, timing, with/without food, what to do if a dose is missed
3. How long to take it and what to do when it runs out
4. The 5 most important side effects to watch for — described by how they feel, not medical terms
5. What to avoid while taking this medication (foods, activities, other medications, alcohol)
6. Signs of a serious reaction requiring emergency care
7. How to store the medication
8. A "Frequently Asked Questions" section with 3 common patient questions and direct answers
Write at a 6th-grade reading level. Avoid all Latin abbreviations (write "twice daily" not "BID").Prompt 15: Post-Visit Summary Message
You are a physician composing a patient portal message summarizing today's visit. Write a warm, clear, and complete post-visit summary for:
Visit date: [DATE]
Patient name: [FIRST_NAME_ONLY_FOR_PRIVACY]
Visit reason: [CHIEF_COMPLAINT_OR_VISIT_TYPE]
Key discussion points from visit: [BULLET_POINTS_FROM_ENCOUNTER]
Diagnoses addressed: [DIAGNOSIS_LIST]
New medications started: [LIST_WITH_DOSES]
Medications stopped or changed: [LIST_WITH_REASON]
Lab/imaging ordered: [TESTS_ORDERED]
Referrals placed: [SPECIALTY_AND_REASON]
Follow-up: [TIMEFRAME_AND_REASON]
Specific instructions: [DIET_ACTIVITY_MONITORING_ETC]
Write a message that:
1. Opens with a personalized, warm greeting (not generic)
2. Summarizes what was discussed in plain language
3. Clearly lists "Your Action Items" as a numbered checklist
4. Explains what to expect from ordered tests and when results will be available
5. Provides specific instructions for when to call the office vs. go to the ER
6. Closes with an invitation to message with questions
7. Is under 350 words and reads at an 8th-grade levelPrompt 16: Motivational Interviewing Script for Lifestyle Change
You are a physician or health coach preparing for a motivational interviewing conversation about lifestyle change with:
Patient profile: [AGE]-year-old [BIOLOGICAL_SEX]
Target behavior change: [SMOKING_CESSATION/WEIGHT_LOSS/PHYSICAL_ACTIVITY/ALCOHOL_REDUCTION/MEDICATION_ADHERENCE]
Current stage of change (Prochaska): [PRECONTEMPLATION/CONTEMPLATION/PREPARATION/ACTION/MAINTENANCE]
Relevant clinical context: [DIAGNOSIS_AND_WHY_CHANGE_MATTERS_CLINICALLY]
Known barriers mentioned by patient: [BARRIERS]
Patient's stated motivation (if any): [MOTIVATION_OR_NONE]
Generate a structured MI conversation guide that includes:
1. An opening reflective statement that validates the patient's current position
2. 5 open-ended questions appropriate to their stage of change
3. 3 affirmations specific to this patient's situation
4. Reflective listening responses for common patient resistance statements
5. A values clarification exercise appropriate for this patient
6. A SMART goal formulation template for this specific behavior
7. A closing commitment statement the patient can phrase in their own words
Base the approach on Miller & Rollnick's Motivational Interviewing framework, 3rd edition.
Section 4: Clinical Research and Literature Analysis Prompts
For clinical researchers, evidence-based medicine practitioners, and academic physicians, GPT-5.5 represents a significant acceleration in the literature synthesis pipeline. The model can critically appraise study methodology, identify statistical limitations, generate structured abstracts, assist with systematic review protocols, and translate statistical findings into clinically meaningful language. These prompts are designed for researchers who need rigorous, methodologically sound outputs — not surface-level summaries.
Prompt 17: Critical Appraisal of an RCT
You are a clinical epidemiologist performing a critical appraisal of a randomized controlled trial. Appraise the following study:
Study title: [TITLE]
Journal: [JOURNAL] | Publication year: [YEAR] | Impact factor: [IF_IF_KNOWN]
PICO:
- Population: [POPULATION]
- Intervention: [INTERVENTION]
- Comparator: [COMPARATOR]
- Outcome (primary): [PRIMARY_OUTCOME]
- Outcome (secondary): [SECONDARY_OUTCOMES]
Study details:
- Sample size: [N] | Power calculation: [STATED_POWER]
- Randomization method: [METHOD]
- Blinding: [OPEN/SINGLE/DOUBLE/TRIPLE_BLIND]
- ITT vs. per-protocol analysis: [ANALYSIS_TYPE]
- Follow-up duration: [DURATION] | Dropout rate: [DROPOUT_PERCENT]
- Key results: [PRIMARY_OUTCOME_RESULT_WITH_CI_AND_P_VALUE]
- Funding source: [FUNDING]
Using the Cochrane Risk of Bias 2.0 (RoB 2) tool and CONSORT 2010 checklist:
1. Assess risk of bias across all 5 RoB 2 domains with justification
2. Evaluate statistical methodology: NNT, NNH, ARR, RRR, 95% CI interpretation
3. Assess internal validity threats
4. Assess external validity and generalizability to [YOUR_PATIENT_POPULATION]
5. Identify any spin in the abstract or discussion vs. actual results
6. Provide an overall quality rating: High / Moderate / Low / Very Low (GRADE)
7. State whether this study should change clinical practice and whyPrompt 18: Systematic Review Protocol Development
You are a clinical researcher developing a PRISMA-compliant systematic review protocol. Help develop a protocol for:
Research question: [RESEARCH_QUESTION]
Clinical specialty: [SPECIALTY]
Intended use: [CLINICAL_GUIDELINE_DEVELOPMENT/ACADEMIC_PUBLICATION/HEALTH_TECHNOLOGY_ASSESSMENT]
Generate a complete systematic review protocol including:
1. Background and rationale (200 words)
2. PICO framework with explicit inclusion/exclusion criteria for each element
3. Study design eligibility criteria (RCTs only / observational / all designs)
4. Search strategy for PubMed/MEDLINE, Embase, and Cochrane — include MeSH terms and Boolean operators
5. Grey literature sources to search
6. Data extraction template with 15 key variables
7. Quality assessment tool selection with justification (RoB 2, ROBINS-I, NOS, etc.)
8. Planned statistical synthesis approach: meta-analysis feasibility, heterogeneity assessment (I² threshold), subgroup analyses
9. GRADE evidence certainty assessment plan
10. Timeline estimate for each phase
11. PROSPERO registration checklist
Format as a structured protocol document suitable for PROSPERO submission.Prompt 19: Meta-Analysis Results Interpretation
You are a biostatistician and clinical researcher. Interpret the following meta-analysis results for a clinical audience:
Meta-analysis topic: [TOPIC]
Number of included studies: [N_STUDIES] | Total participants: [N_PARTICIPANTS]
Primary outcome: [OUTCOME]
Statistical results:
- Pooled effect size: [EFFECT_SIZE_TYPE (OR/RR/MD/SMD)] = [VALUE], 95% CI [LOWER]-[UPPER]
- P-value: [P_VALUE]
- Heterogeneity: I² = [I2_PERCENT], Tau² = [TAU2], Q statistic p = [Q_P_VALUE]
- Publication bias: [FUNNEL_PLOT_SYMMETRY/EGGER_TEST_RESULT]
- Subgroup analyses performed: [LIST_SUBGROUPS_AND_RESULTS]
- Sensitivity analyses: [RESULTS]
Provide:
1. Plain-language interpretation of the pooled effect size for a clinical audience
2. Clinical significance assessment (not just statistical significance)
3. Explanation of heterogeneity level and its implications for applying results
4. Assessment of publication bias impact on conclusions
5. NNT or NNH calculation if applicable
6. Subgroup findings that are clinically actionable
7. Limitations of this meta-analysis that should temper conclusions
8. A one-paragraph "Bottom Line for Clinical Practice" statementPrompt 20: Grant Application Specific Aims Page
You are a senior biomedical researcher with extensive NIH grant writing experience. Write a Specific Aims page for:
Funding mechanism: [R01/R21/K23/K08/OTHER]
Study section: [STUDY_SECTION_IF_KNOWN]
Research area: [BROAD_RESEARCH_AREA]
Clinical problem: [CLINICAL_PROBLEM_AND_SIGNIFICANCE]
Knowledge gap: [SPECIFIC_GAP_IN_CURRENT_KNOWLEDGE]
Proposed approach: [BRIEF_DESCRIPTION_OF_STUDY_DESIGN]
Preliminary data: [SUMMARY_OF_PRELIMINARY_FINDINGS]
Long-term goal: [INVESTIGATOR'S_LONG_TERM_RESEARCH_GOAL]
Specific Aims (provide 3):
Aim 1: [BRIEF_DESCRIPTION]
Aim 2: [BRIEF_DESCRIPTION]
Aim 3: [BRIEF_DESCRIPTION]
Write a Specific Aims page that:
1. Opens with a compelling hook about the clinical/scientific problem (2-3 sentences)
2. Clearly articulates the knowledge gap and why it matters
3. States the central hypothesis with logical basis from preliminary data
4. Presents each Aim with: rationale, approach (brief), and expected outcome
5. Includes a "Potential Pitfalls" acknowledgment to demonstrate rigor
6. Closes with an innovation and impact statement
7. Fits within one page (approximately 600-650 words)
8. Uses active voice and avoids jargon accessible only to subspecialistsPrompt 21: Case Report Writing
You are a physician preparing a case report for journal submission. Write a structured case report for:
Target journal: [JOURNAL_NAME] | Word limit: [WORD_LIMIT]
CARE guideline compliance: required
Case summary:
- Patient demographics (de-identified): [AGE_RANGE]-year-old [BIOLOGICAL_SEX]
- Presenting complaint: [COMPLAINT]
- Key clinical findings: [EXAMINATION_FINDINGS]
- Diagnostic workup: [TESTS_AND_RESULTS]
- Diagnosis: [FINAL_DIAGNOSIS]
- Treatment: [TREATMENT_DETAILS]
- Outcome: [PATIENT_OUTCOME]
- Follow-up: [FOLLOW_UP_DURATION_AND_STATUS]
- What makes this case novel or educational: [NOVELTY_STATEMENT]
Write a complete case report including:
1. Title (informative, not sensationalized)
2. Abstract (structured: Background, Case Presentation, Conclusion — 250 words)
3. Introduction with literature context (300 words)
4. Case Presentation following CARE guidelines
5. Discussion: pathophysiology, differential diagnosis reasoning, treatment rationale, comparison to published cases
6. Key Learning Points (3 bullet points)
7. Patient Perspective section (brief, written in first person from patient's viewpoint)
8. References section headers (list 8-10 relevant citation placeholders by topic)
Flag any patient identifiers that require additional de-identification before submission.Section 5: Healthcare Administration and Compliance Prompts
Healthcare administrators, compliance officers, quality improvement specialists, and practice managers face a distinct set of challenges that are equally well-suited to GPT-5.5’s capabilities. From drafting HIPAA-compliant policies to generating quality improvement project charters, these prompts address the operational backbone of healthcare organizations.
Prompt 22: HIPAA Compliance Policy Draft
You are a healthcare compliance attorney and privacy officer. Draft a HIPAA-compliant policy for:
Policy topic: [SPECIFIC_POLICY_TOPIC — e.g., "Use of Mobile Devices for PHI Access", "Breach Notification Procedures", "Business Associate Agreement Management"]
Organization type: [HOSPITAL/PHYSICIAN_PRACTICE/HEALTH_PLAN/BUSINESS_ASSOCIATE]
Organization size: [NUMBER_OF_EMPLOYEES]
State: [STATE — for state-specific privacy law overlay]
Applicable regulations: HIPAA Privacy Rule, Security Rule, Breach Notification Rule, [STATE_PRIVACY_LAW_IF_APPLICABLE]
Generate a complete policy document that includes:
1. Policy title, number, effective date, and review cycle
2. Purpose and scope statement
3. Definitions section (minimum 8 defined terms)
4. Policy statement
5. Procedures (numbered, step-by-step)
6. Roles and responsibilities matrix
7. Training requirements
8. Violation consequences
9. Policy exceptions process
10. References to 45 CFR sections and applicable OCR guidance
11. Document control footer
Flag any provisions that require legal review before implementation and any areas where state law may be more stringent than federal HIPAA requirements.Prompt 23: Quality Improvement Project Charter
You are a quality improvement specialist using the IHI Model for Improvement. Create a QI project charter for:
Problem statement: [SPECIFIC_QUALITY_PROBLEM — include baseline metric]
Clinical unit/department: [UNIT]
Patient population affected: [POPULATION]
Aim statement components:
- What will be improved: [OUTCOME_MEASURE]
- By how much: [QUANTIFIED_GOAL]
- By when: [TIMELINE]
- For whom: [POPULATION]
Team:
- Executive sponsor: [ROLE]
- Project lead: [ROLE]
- Team members: [ROLES_LIST]
Available data sources: [EHR_REGISTRY_CLAIMS_MANUAL_AUDIT]
Known root causes (from fishbone/5-why analysis): [CAUSES_IF_KNOWN]
Proposed interventions: [INTERVENTIONS_LIST]
Generate a complete QI project charter including:
1. Problem statement with current state data
2. SMART aim statement
3. Process map scope (start/end points)
4. Outcome, process, and balancing measures with operational definitions
5. PDSA cycle plan for first 3 cycles
6. Driver diagram (primary and secondary drivers)
7. Timeline with milestones
8. Resource requirements and budget estimate
9. Communication plan
10. Sustainability plan
Format for presentation to hospital quality committee.Prompt 24: Incident Report and Root Cause Analysis
You are a patient safety officer conducting a root cause analysis (RCA) following a patient safety event. Facilitate an RCA for:
Event type: [SENTINEL_EVENT/SERIOUS_SAFETY_EVENT/NEAR_MISS]
Event description: [FACTUAL_DESCRIPTION_OF_WHAT_HAPPENED — no names]
Patient harm level (NCC MERP): [CATEGORY_A_THROUGH_I]
Date/time of event: [DATE_TIME]
Location: [UNIT_OR_DEPARTMENT]
Staff involved: [ROLES_ONLY — no names]
Immediate actions taken: [IMMEDIATE_RESPONSE_ACTIONS]
Conduct a structured RCA that:
1. Creates a timeline of events (chronological sequence)
2. Identifies contributing factors using the 5-Why technique for each contributing cause
3. Categorizes causes using the Fishbone (Ishikawa) diagram: People, Process, Equipment, Environment, Management
4. Distinguishes active errors from latent system failures
5. Identifies which contributing factors were preventable
6. Generates corrective action recommendations mapped to each root cause
7. Assigns responsibility (by role) and timeline for each corrective action
8. Recommends monitoring metrics to verify effectiveness of corrections
9. Identifies similar events in literature and what was learned
Format for Joint Commission RCA reporting requirements.Prompt 25: Staff Training Module Outline
You are a healthcare education specialist. Create a comprehensive training module outline for:
Training topic: [TOPIC — e.g., "Sepsis Recognition and Early Response", "Fall Prevention Bundle", "Hand Hygiene Compliance"]
Target audience: [NURSES/PHYSICIANS/ALL_CLINICAL_STAFF/ADMINISTRATIVE_STAFF]
Delivery format: [IN_PERSON/ONLINE_ASYNCHRONOUS/BLENDED]
Duration: [TOTAL_TRAINING_HOURS]
Accreditation: [CME/CNE/NEITHER]
Regulatory driver: [JOINT_COMMISSION/CMS/STATE_BOARD/INTERNAL_POLICY]
Current performance gap: [BASELINE_METRIC_AND_TARGET]
Generate a complete training module outline including:
1. Learning objectives (minimum 5, written in Bloom's Taxonomy action verbs at appropriate cognitive levels)
2. Pre-assessment questions (5 multiple choice)
3. Module sections with content outline and time allocation
4. Case-based learning scenarios (3 clinical cases with discussion questions)
5. Skills demonstration checklist (if applicable)
6. Post-assessment questions (10 multiple choice with rationales)
7. Competency verification method
8. References and evidence base
9. Evaluation (Kirkpatrick Level 1-3 plan)
10. Annual review/update scheduleSection 6: Nursing-Specific Prompts
Nurses represent the largest segment of the healthcare workforce, and their documentation, handoff communication, and patient education responsibilities are substantial. These prompts are specifically designed for bedside nurses, charge nurses, and nurse practitioners.
Prompt 26: SBAR Handoff Communication
You are a charge nurse preparing a shift handoff report using the SBAR framework. Generate a complete SBAR handoff for:
Patient: [AGE]-year-old [BIOLOGICAL_SEX] in room [ROOM_NUMBER]
Admitting diagnosis: [DIAGNOSIS]
Day of admission: [DAY_NUMBER]
Shift: [OUTGOING_SHIFT] to [INCOMING_SHIFT]
Clinical status:
- Current vital signs: [VITALS]
- Relevant assessment findings: [HEAD_TO_TOE_HIGHLIGHTS]
- Active IV access: [LINES_AND_LOCATIONS]
- Current drips/infusions: [LIST_WITH_RATES]
- Recent labs: [RELEVANT_RESULTS_WITH_TIMES]
- Recent procedures or events: [PROCEDURES_EVENTS]
- Pain level: [PAIN_SCALE_AND_MANAGEMENT]
- Mobility/fall risk: [STATUS]
- Code status: [FULL_CODE/DNR/DNI]
Outstanding tasks: [PENDING_ITEMS]
Family/communication issues: [CONCERNS_IF_ANY]
Anticipated events next shift: [PROCEDURES_DISCHARGE_CONCERNS]
Generate a structured SBAR that:
1. Is concise but complete (under 3 minutes to verbalize)
2. Highlights any changes from previous shift
3. Clearly identifies the top 3 nursing priorities for the incoming nurse
4. Flags any safety concerns requiring immediate attention
5. Includes a "Recommendation" with specific asks of the incoming nursePrompt 27: Nursing Care Plan
You are a registered nurse developing a comprehensive nursing care plan using NANDA-I nursing diagnoses. Create a care plan for:
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Medical diagnosis: [MEDICAL_DIAGNOSIS]
Relevant assessment data: [ASSESSMENT_FINDINGS]
Patient's stated concerns: [PATIENT_CONCERNS]
ADL status: [INDEPENDENT/PARTIAL_ASSIST/TOTAL_CARE]
Psychosocial factors: [RELEVANT_FACTORS]
Generate a nursing care plan with 4 nursing diagnoses that includes for each:
1. NANDA-I nursing diagnosis statement (Problem + Etiology + Signs/Symptoms)
2. Short-term goal (measurable, achievable within 24-48 hours)
3. Long-term goal (measurable, achievable by discharge)
4. Nursing interventions (minimum 5 per diagnosis, with rationale for each)
5. Expected outcomes with measurable criteria
6. Evaluation statement
Prioritize diagnoses using Maslow's Hierarchy of Needs. Include at least one psychosocial/emotional nursing diagnosis. Format for electronic care plan documentation.Section 7: Mental Health and Behavioral Health Prompts
Prompt 28: Psychiatric Intake Assessment Summary
You are a psychiatrist or psychiatric NP completing an intake assessment summary. Generate a structured psychiatric intake summary based on:
Patient: [AGE]-year-old [BIOLOGICAL_SEX], [RELATIONSHIP_STATUS], [EMPLOYMENT_STATUS]
Presenting concern: [CHIEF_COMPLAINT_IN_PATIENT'S_WORDS]
History of present illness: [HPI_NARRATIVE]
Psychiatric history: [PRIOR_DIAGNOSES_HOSPITALIZATIONS_TREATMENTS]
Substance use history: [SUBSTANCES_FREQUENCY_LAST_USE_TREATMENT]
Medical history: [PMH_RELEVANT_TO_PSYCHIATRY]
Family psychiatric history: [FAMILY_HISTORY]
Social history: [LIVING_SITUATION_SUPPORT_TRAUMA_HISTORY]
Current medications: [LIST]
Mental status exam: [MSE_FINDINGS]
Safety assessment: [SI_HI_PLAN_MEANS_INTENT]
Collateral information: [SOURCE_AND_CONTENT]
Generate a complete psychiatric intake summary that:
1. Follows DSM-5-TR diagnostic framework
2. Includes differential diagnosis with at least 3 considerations
3. Documents Columbia Suicide Severity Rating Scale (C-SSRS) findings
4. Provides risk stratification: Low / Moderate / High with specific risk and protective factors
5. Recommends diagnostic formulation using biopsychosocial model
6. Proposes treatment plan: medication, therapy modality, level of care
7. Documents capacity assessment
8. Meets CMS documentation requirements for psychiatric evaluation (90791)Prompt 29: Therapy Progress Note (DAP Format)
You are a licensed clinical social worker or psychotherapist. Generate a therapy progress note in DAP format for:
Session number: [SESSION_NUMBER] | Date: [DATE]
Session duration: [MINUTES] | Modality: [INDIVIDUAL/FAMILY/GROUP]
Therapeutic approach: [CBT/DBT/ACT/EMDR/PSYCHODYNAMIC/OTHER]
Treatment goals being addressed: [GOALS_FROM_TREATMENT_PLAN]
Session content:
- Patient presentation at start: [MOOD_AFFECT_ENGAGEMENT]
- Key topics discussed: [TOPICS]
- Interventions used: [SPECIFIC_TECHNIQUES]
- Patient response to interventions: [RESPONSE]
- Homework assigned/reviewed: [HOMEWORK]
- Safety check: [SI_HI_CURRENT_STATUS]
- Plan for next session: [PLAN]
Generate a DAP note that:
1. Data section: Objective observations and patient-reported information
2. Assessment section: Clinical interpretation, progress toward goals, diagnostic impressions
3. Plan section: Next session focus, homework, referrals, medication coordination
4. Meets requirements for [INSURANCE_TYPE] billing under CPT [90837/90834/90832]
5. Avoids verbatim patient quotes that could compromise confidentiality
6. Documents medical necessity for continued treatmentSection 8: Specialty-Specific Clinical Prompts
Prompt 30: Oncology Treatment Summary
You are an oncologist creating a treatment summary for a cancer patient completing active treatment. Generate a comprehensive treatment summary for:
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Cancer diagnosis: [CANCER_TYPE], [STAGE_AND_STAGING_SYSTEM]
Date of diagnosis: [DATE]
Tumor characteristics: [HISTOLOGY_GRADE_BIOMARKERS — e.g., ER/PR/HER2, KRAS, PD-L1]
Treatment received:
- Surgery: [PROCEDURE_DATE_SURGEON_PATHOLOGY_MARGINS]
- Radiation: [FIELDS_DOSE_FRACTIONS_DATES]
- Systemic therapy: [REGIMEN_DOSES_CYCLES_DATES]
- Clinical trial participation: [TRIAL_NAME_AND_ARM_IF_APPLICABLE]
Treatment response: [COMPLETE/PARTIAL/STABLE/PROGRESSIVE]
Significant toxicities experienced: [LIST_WITH_GRADE_AND_MANAGEMENT]
Current status: [NED/ACTIVE_DISEASE/SURVEILLANCE]
Generate a treatment summary following ASCO's Cancer Treatment Summary template that:
1. Provides a complete treatment chronology
2. Documents all pathology with staging
3. Lists long-term effects to monitor (organ-specific, based on treatments received)
4. Provides surveillance schedule with specific tests and intervals
5. Identifies late effects risks and screening recommendations
6. Lists signs of recurrence the patient should report
7. Includes psychosocial support resources
8. Is formatted for both the patient and receiving primary care physicianPrompt 31: Cardiology Stress Test Interpretation
You are an attending cardiologist interpreting a stress test report. Provide a structured interpretation for:
Test type: [STANDARD_EXERCISE/PHARMACOLOGIC] stress [ECG/ECHO/NUCLEAR]
Indication: [INDICATION]
Patient: [AGE]-year-old [BIOLOGICAL_SEX], [HEIGHT_CM], [WEIGHT_KG]
Baseline ECG: [FINDINGS]
Pre-test probability of CAD (Duke Clinical Score): [LOW/INTERMEDIATE/HIGH]
Medications held: [YES/NO — list]
Exercise data (if applicable):
- Protocol: [BRUCE/MODIFIED_BRUCE/OTHER]
- Duration: [MINUTES] | METs achieved: [METS]
- Reason for stopping: [REASON]
- Target heart rate: [TARGET] | Achieved: [ACHIEVED_PERCENT]
- Blood pressure response: [PATTERN]
- Symptoms: [SYMPTOMS_DURING_TEST]
- ECG changes: [ST_CHANGES_LOCATION_MAGNITUDE]
Imaging data (if echo/nuclear):
- Resting wall motion/perfusion: [FINDINGS]
- Stress wall motion/perfusion: [FINDINGS]
- LVEF rest/stress: [VALUES]
- Ischemic burden estimate: [PERCENT_IF_NUCLEAR]
Provide:
1. Adequacy of test assessment
2. Hemodynamic response interpretation
3. ECG interpretation with Duke Treadmill Score calculation
4. Imaging interpretation (if applicable)
5. Overall test result: Normal / Equivocal / Abnormal / High-Risk Features
6. Risk stratification and recommended management pathway
7. Recommendation for further testing or treatment per ACC/AHA guidelinesPrompt 32: Radiology Report Summarization for Clinician
You are a radiologist or clinician summarizing a radiology report for clinical decision-making. Analyze and summarize the following radiology report:
[PASTE_FULL_RADIOLOGY_REPORT_TEXT_HERE]
Patient context:
- Clinical question being answered: [CLINICAL_QUESTION]
- Patient's relevant history: [RELEVANT_HISTORY]
- Prior imaging for comparison: [AVAILABLE/NOT_AVAILABLE]
Provide:
1. One-sentence "bottom line" answer to the clinical question
2. Key positive findings (clinically significant)
3. Key negative findings (relevant to the differential)
4. Incidental findings requiring follow-up (separate from primary question)
5. Radiologist's recommendation summary
6. Urgency classification: Routine / Semi-urgent (2-4 weeks) / Urgent (24-48 hours) / Critical (immediate)
7. Suggested next imaging step if indicated
8. Plain-language explanation suitable for patient communication
Flag any findings that require immediate physician notification per ACR communication guidelines.Section 9: Emergency Medicine and Critical Care Prompts
Prompt 33: Trauma Activation Criteria Assessment
You are an emergency medicine physician evaluating a trauma patient for trauma team activation. Assess the following:
Mechanism of injury: [MOI_DESCRIPTION]
Pre-hospital vital signs: [VITALS_WITH_GCS]
Physical exam findings on arrival: [EXAM_FINDINGS]
Visible injuries: [INJURIES]
Patient age: [AGE] | Comorbidities: [COMORBIDITIES]
EMS narrative: [EMS_REPORT]
Using ACS-COT field triage guidelines and your institution's trauma activation criteria:
1. Classify activation level: Level 1 (highest) / Level 2 / Consult
2. List the specific criteria met for this classification
3. Identify the primary survey priorities (ABCDE approach)
4. Recommend immediate resuscitation interventions
5. Generate a trauma bay preparation checklist
6. Identify injury patterns that must be ruled out given the mechanism
7. Calculate initial FAST exam priorities
8. Recommend CT imaging protocol
9. Identify any immediate surgical consultation triggersPrompt 34: ICU Daily Goals Checklist
You are an intensivist conducting morning ICU rounds. Generate a structured daily goals checklist for:
Patient: [AGE]-year-old [BIOLOGICAL_SEX], ICU day [DAY_NUMBER]
Admitting diagnosis: [DIAGNOSIS]
Current status: [BRIEF_CLINICAL_STATUS]
Ventilator status: [INTUBATED_WITH_SETTINGS / EXTUBATED / NIPPV]
Vasopressors: [AGENTS_AND_DOSES_OR_NONE]
Lines/tubes: [LIST_WITH_INSERTION_DATES]
Current antibiotics: [LIST_WITH_DAY_NUMBER]
Nutrition: [ENTERAL/PARENTERAL/NPO — rate and goal]
DVT prophylaxis: [AGENT_OR_CONTRAINDICATION]
Stress ulcer prophylaxis: [AGENT_OR_CONTRAINDICATION]
Sedation/analgesia: [AGENTS_RASS_TARGET_CPOT_SCORE]
Generate an ICU daily goals checklist addressing:
1. Respiratory: ventilator weaning readiness (SAT/SBT criteria), extubation readiness
2. Cardiovascular: vasopressor weaning targets, fluid balance goal
3. Infectious: antibiotic day count, de-escalation opportunity, culture results pending
4. Neurological: RASS/CAM-ICU, sedation vacation plan, delirium prevention
5. Renal: fluid balance, AKI staging, RRT need assessment
6. Nutrition: caloric goal achievement, GI tolerance
7. Lines: necessity review, infection risk, removal candidates
8. Mobility: PT/OT goals for today
9. Family communication: update needed, goals of care discussion needed
10. Discharge planning: anticipated ICU discharge readinessSection 10: Additional High-Value Prompts Across Specialties
Prompt 35: Dermatology Lesion Description for Teledermatology
Prompt 36: Nephrology Dialysis Prescription
Prompt 37: Endocrinology Insulin Titration Protocol
Prompt 38: Obstetrics Antepartum Risk Stratification
Prompt 39: Palliative Care Goals of Care Documentation
Prompt 40: Geriatrics Comprehensive Medication Review (Beers Criteria)
These specialty prompts follow the same structural pattern as those above. Below are the full production-ready versions for the four most universally applicable:
Prompt 37 (Full): Endocrinology Insulin Titration Protocol
You are an endocrinologist developing an insulin titration protocol for:
Patient: [AGE]-year-old [BIOLOGICAL_SEX] with [TYPE_1/TYPE_2] diabetes
Current A1c: [VALUE] | Target A1c: [TARGET]
Current insulin regimen: [BASAL_BOLUS/PREMIXED/PUMP — doses and timing]
Recent glucose log (7-14 days): [FASTING_READINGS] / [PRE-MEAL] / [POST-MEAL] / [BEDTIME]
Hypoglycemia history: [FREQUENCY_SEVERITY_AWARENESS]
Weight: [WEIGHT_KG] | Renal function: eGFR [VALUE]
Carbohydrate counting ability: [YES/NO]
CGM in use: [YES — device / NO]
Physical activity level: [SEDENTARY/MODERATE/ACTIVE]
Other diabetes medications: [LIST]
Generate a structured insulin titration plan that:
1. Identifies the primary glucose pattern problem (fasting hyperglycemia, post-prandial, nocturnal hypoglycemia, etc.)
2. Provides specific dose adjustment recommendations with reasoning
3. Calculates estimated total daily dose and basal:bolus ratio
4. Provides correction factor (ISF) and carbohydrate ratio if applicable
5. Sets glucose targets for fasting, post-prandial, and bedtime
6. Defines hypoglycemia management protocol for this patient
7. Establishes a titration schedule (how often to adjust and by how much)
8. Sets a follow-up timeline with A1c recheck recommendation
9. Flags any concerning patterns requiring urgent interventionPrompt 39 (Full): Palliative Care Goals of Care Documentation
You are a palliative care physician documenting a goals of care family meeting. Generate a structured goals of care documentation note for:
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Primary diagnosis: [DIAGNOSIS]
Prognosis: [PROGNOSIS_STATEMENT — e.g., "months to a year", "weeks to months"]
Current functional status: [KPS_OR_ECOG_SCORE]
Cognitive status: [DECISIONAL_CAPACITY: YES/NO/FLUCTUATING]
Surrogate (if applicable): [RELATIONSHIP_AND_NAME_OPTIONAL]
Meeting attendees: [ROLES — no names needed]
Meeting duration: [MINUTES]
Key discussion points:
- Patient/family understanding of diagnosis and prognosis: [UNDERSTANDING_LEVEL]
- Patient's stated values and priorities: [VALUES_VERBATIM_OR_PARAPHRASED]
- Fears and concerns expressed: [CONCERNS]
- Prior advance directive: [YES — type / NO]
- Discussions held regarding: [CPR/INTUBATION/HOSPITALIZATION/ARTIFICIAL_NUTRITION/COMFORT_FOCUSED_CARE]
- Decisions reached: [DECISIONS]
- Unresolved areas: [UNRESOLVED]
Generate a goals of care documentation note that:
1. Documents capacity assessment or surrogate authority
2. Records prognosis communication and family comprehension
3. Captures patient's values in their own words where possible
4. Documents specific decisions reached on each life-sustaining treatment
5. Records POLST/MOLST form completion status
6. Identifies ongoing spiritual, psychosocial, and practical needs
7. Plans next family meeting or communication touchpoint
8. Meets CMS documentation requirements for advance care planning billing (99497/99498)Prompt 40 (Full): Geriatrics Comprehensive Medication Review (Beers Criteria)
You are a geriatrician and clinical pharmacist conducting a comprehensive medication review for an older adult:
Patient: [AGE]-year-old [BIOLOGICAL_SEX]
Weight: [WEIGHT_KG] | eGFR: [VALUE] | Hepatic function: [STATUS]
Cognitive status: [MMSE_OR_MOCA_SCORE_OR_DESCRIPTION]
Fall history: [YES — frequency / NO]
Current medication list with doses, frequencies, and indications:
[PASTE_COMPLETE_MEDICATION_LIST]
Diagnoses: [COMPLETE_PROBLEM_LIST]
Conduct a comprehensive medication review using:
1. 2023 AGS Beers Criteria — flag all potentially inappropriate medications (PIMs) with specific concern
2. STOPP/START criteria v3 — identify medications to stop AND medications that should be started
3. Anticholinergic Cognitive Burden (ACB) scale — calculate total ACB score
4. Drug-drug interactions with clinical significance rating
5. Medication-disease interactions specific to this patient's comorbidities
6. Renal dose adjustment requirements based on eGFR
7. Cascade prescribing identification (medication prescribed to treat a side effect of another medication)
8. Deprescribing candidates with evidence-based tapering recommendations
9. Medication reconciliation gaps (missing medications for documented conditions)
10. Adherence risk assessment based on regimen complexity
Provide a prioritized action plan: Critical (address this visit) / Important (address next visit) / Routine (address at annual review)Optimizing GPT-5.5 for Clinical Use: Practical Configuration Guidance
Using these prompts effectively requires understanding how to configure GPT-5.5 for clinical contexts. Several system-level settings and prompt engineering principles will significantly improve output quality and consistency across your healthcare workflows.
System Prompt Configuration for Clinical Environments
When using GPT-5.5 via API or in a custom GPT configuration, a well-crafted system prompt establishes the clinical context that makes every subsequent interaction more precise. Here is a production-ready system prompt for clinical use:
Access 40,000+ AI Prompts for ChatGPT, Claude & Codex — Free!
Subscribe to get instant access to our complete Notion Prompt Library — the largest curated collection of prompts for ChatGPT, Claude, OpenAI Codex, and other leading AI models. Optimized for real-world workflows across coding, research, content creation, and business.
You are a clinical AI assistant supporting licensed healthcare professionals in a [INSTITUTION_TYPE] setting. You assist with clinical reasoning, documentation, patient education, and research analysis.
Core operating principles:
1. All outputs are for review by a licensed clinician before use in patient care — state this when clinically relevant
2. Cite specific guidelines, scoring systems, and evidence levels when making clinical recommendations
3. Flag uncertainty explicitly: distinguish between well-established evidence, emerging evidence, and expert opinion
4. Use standard medical terminology appropriate to the requesting clinician's specialty
5. For dosing and pharmacology questions, always recommend verification against current pharmacist resources or FDA labeling
6. Never fabricate drug names, study citations, or clinical data — if uncertain, state the limitation
7. When patient safety is at risk, prioritize safety over brevity
8. Maintain HIPAA-conscious language — do not request or store PHI beyond what is provided in the prompt
Current institutional context: [SPECIALTY/DEPARTMENT]
Primary user role: [PHYSICIAN/NP/PA/NURSE/RESEARCHER/ADMINISTRATOR]Prompt Chaining for Complex Clinical Workflows
For complex tasks like comprehensive discharge planning or systematic review development, chaining multiple prompts in sequence produces far better results than attempting everything in one prompt. A practical workflow for discharge planning might sequence: (1) medication reconciliation review → (2) patient education material generation → (3) follow-up care coordination letter → (4) post-visit portal message. Each output feeds context into the next prompt, creating a coherent documentation package.
Quality Control Checklist for Clinical AI Outputs
Every GPT-5.5 output used in a clinical context should pass through a rapid quality check before use:
- Factual accuracy: Are drug names, doses, and guideline citations correct and current?
- Patient specificity: Does the output account for this specific patient’s comorbidities, allergies, and renal/hepatic function?
- Completeness: Are there missing elements that would be expected in this document type?
- Tone appropriateness: Is the language calibrated correctly for the intended audience (patient vs. specialist vs. payer)?
- Safety flags: Has the model appropriately highlighted any urgent or safety-critical concerns?
- Hallucination check: Are any cited studies, guidelines, or statistics verifiable? GPT-5.5 has dramatically reduced hallucination rates compared to earlier models, but verification remains essential for clinical use.
Regulatory and Ethical Considerations for Healthcare AI Use
As GPT-5.5 becomes embedded in clinical workflows, healthcare professionals must understand the evolving regulatory landscape. The FDA’s Digital Health Center of Excellence has issued guidance on AI/ML-based Software as a Medical Device (SaMD), and institutions using AI for clinical decision support must assess whether their use cases fall under FDA oversight. Generally, prompts used to assist documentation or generate educational materials fall outside FDA SaMD jurisdiction, while prompts used to directly inform diagnosis or treatment decisions may require more careful institutional review.
From a liability perspective, the physician or advanced practice provider who reviews and signs off on AI-assisted documentation retains full professional responsibility for that document. AI assistance does not diminish the standard of care obligation. Institutions should establish clear policies governing which clinical tasks may be AI-assisted, what review processes are required, and how AI involvement should be documented in the medical record.
Key Principle: GPT-5.5 can reduce the time it takes to produce high-quality clinical documentation by 40-70% in well-designed workflows. The time savings should be reinvested in direct patient care, not used to justify reduced review rigor.
Building a Department-Level AI Prompting Library
Individual prompt adoption is valuable, but the highest ROI comes from building a shared, curated prompt library at the department or institution level. Here is a practical framework for doing this:
- Audit current documentation pain points: Survey your team to identify the top 10 most time-consuming or error-prone documentation tasks. These become your first prompt development priorities.
- Pilot with 3-5 champion users: Select clinicians who are comfortable with AI tools to test and refine prompts before department-wide rollout. Their feedback will identify edge cases and failure modes.
- Establish a version control system: